SPONDYLOLYSIS: BACKGROUND
What is spondylolysis? |
What is NOT spondylolysis? |
|
Spondylolysis (spon’di-lol’i-sis)
derives from the Greek words “spondulos,” meaning vertebra, and “lusis,”
meaning loosening or unbinding. It describes a condition where there is a bony
defect or fracture in the pars interarticularis (literally the
part between the [facet] joints) of the vertebral arch of the spine. Spondylolysis has been found in approximately
one-half of all young athlete patients complaining of low back pain (98) and it
is considered by many clinicians to be the most
common cause of low back pain in adolescent patients (43).
|
Spondylolysis is NOT spondylosis or
spondylolisthesis. Spondylosis is an
age-related condition of bony overgrowths on vertebrae; it is usually
asymptomatic. Spondylolisthesis can
result when bilateral spondylolysis allows the vertebra to slip forward from one
another. After adolescence, only a small portion of spondylolysis cases (15%)
progress to spondylolisthesis (109). Although there are similarities between
the two conditions, all of the research
presented in this website is intended to address cases of spondylolysis and NOT spondylolisthesis.
|
Who are aesthetic athletes?
Aesthetic athletes are athletes who participate in sports where their performance is explicitly contingent upon appearance. Most notably, these are: gymnastics, diving, skating, and dancing. Spondylolysis is three to ten times more common in aesthetic athletes than the general population (98). Roughly two-thirds of these cases will present with lower back pain and/or sciatica (see Signs and Symptoms, below, 98). Aesthetic sports involve repetitive hyperextension and rotation of the lower (lumbar) spine, which makes it more susceptible to spinal injury (98).
Tell me about the spine
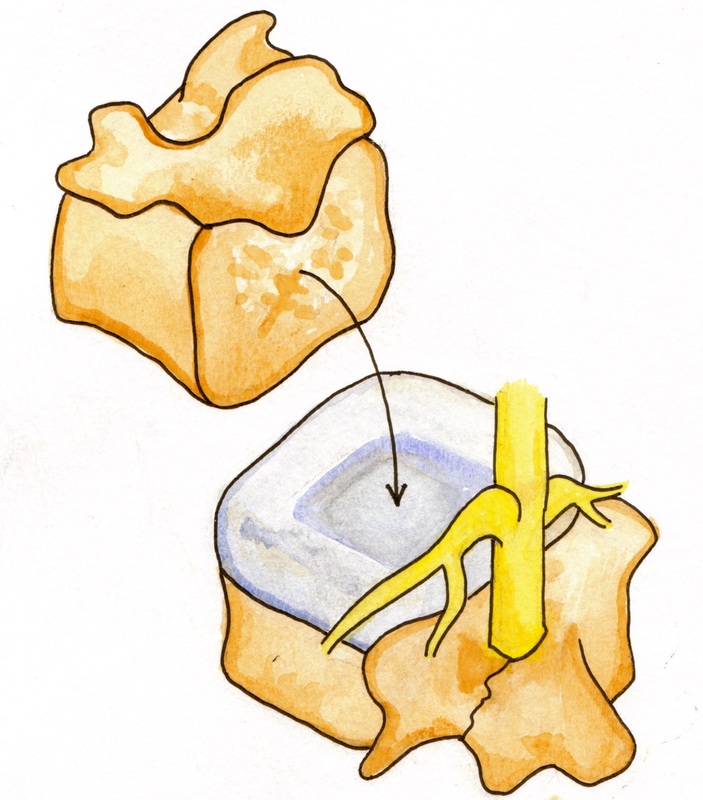
Illustration of two lumbar vertebrae, where the lower vertebrae (depicted with blue intervertebral disc and yellow spinal cord with exiting and entering nerves) has a pars defect on the left pars interarticularis.
|
The spine provides the structural framework for humans to achieve upright posture and motion. It is usually divided into its four primary curves: the cervical (concave), thoracic (convex), lumbar (concave), and sacral/coccyx (convex) curvatures, described in descending location.
The lumbar (lower) spine has five vertebrae. Each of these vertebrae is separated by intervertebral discs that cushion the bodies. Behind each of the vertebral bodies is a bony ring (lamina) that forms a hole (neural foramen) to protect our spinal cord, adjacent blood supply, and exiting and entering nerves. The bony ring also has seven main processes:
|
Spine defects usually occur in the L5 or L4 vertebra (60), which are the lowest two vertebrae of the lumbar spine. When both sides of the pars interarticularis are fractured (a bilateral defect), the inferior articular processes, lamina, and spinous process are physically separated from the superior articular process, pedicles, transverse process, and vertebral body. A weak fibrous connection forms at the site of defect. This weak soft tissue connection may be sufficient for healing (102). It also, however, brings additional nerve elements that increase pain as a method of monitoring stability to protect the spine (36).
Fun Fact: In a lumbar oblique x-ray, spondylolysis classically presents as a “Scotty Dog” collar. The pars defect appears as a collar on the neck (pars interarticularis) of a scotty dog. The scotty dog is formed by the outline of the superior articular process (ear), pedicle (eye/head), transverse process (nose), lamina (body), spinous process (body/tail), and inferior articular processes (legs).
SPONDYLOLYSIS: THE CONDITION
Signs & Symptoms
#1 |
The most common symptom of spondylolysis is localized low back pain (58). Athletes describe the pain using words like “chronic,” “dull,” “achy,” “recurrent,” “constant,” or “catching” (44, 69).
Usually, the pain worsens with activity, especially during hyperextension or activity mimicking sport movements (58). In gymnastics, walkovers, handsprings, rebounds, punching skills, dismount landings, and back twists have been reported to worsen pain (53). Although not yet reported in peer-reviewed research, similar loadings in other sports may also produce pain. Divers, for example may feel more pain during unaligned water entries and forward, inward, and back twisting skills. |
#2 |
The second most common symptom of spondylolysis is sciatica of the L5 or L4 nerve root (22).
The majority will not experience nerve irritation, but those who do may feel pain, numbness, or “pins and needles” sensation in the areas (dermatome) with which the nerve connects. For example, if the L5 nerve root is affected, one may feel tingling along the leg from the outside of the knee down the shin and across to the big toe. If the L4 nerve root is affected, there may be symptoms radiating across the front upper leg (outside to inside), and down the inside of the shin or calf. |
Red Flags
In a clinical examination, “Red flags” indicating a more serious diagnosis must be ruled out. In the younger population, especially:
- Any history of cancer, night pain, pain at rest, unexplained weight loss, or failure to improve (metastatic cancer flags);
- Immunosuppression, prolonged high fever, or history of IV drug abuse, recent urinal tract infection, cellulitis or pneumonia (diskitis or osteomyelitis flags);
- Recent major trauma or prolonged use of corticosteroids (vertebral fracture flags);
- Pulsating mass in the abdomen, throbbing resting back pain, or history of artherosclerotic vascular disease (abdominal aortic aneurysm flags).
DiagnosisAfter taking a history, a doctor will usually perform a physical examination. People with spondylolysis often have tenderness above the defect, muscle spasm, hamstring tightness, and relatively limited range of motion with back extension and single leg hyperextension (58).
Spondylolysis symptoms may appear similar to other low back causes, so X-rays can be taken to confirm presence of the lower vertebrae pars defect of spondylolysis. Single-photon emissions computed tomography (SPECT), computed tomography (CT), and magnetic resonance imaging (MRI) may also be used to detect smaller defects, visualize surrounding soft tissue, or provide a more accurate staging of the spondylolysis (51). Spinal abnormalities are relatively common, however, and the presence of an abnormality does not necessarily mean that the defect is causing the low back pain. |
PrognosisOver 80% of children non-surgically treated will recover within six months of treatment onset (42). Bony healing estimates propose that 75-100% of acute lesions heal, 50% of bilateral acute lesions (fracture on both pars interarticularis sides) heal, and no chronic defects heal, though fibrous union may be acceptable for recovery (42).
|